One of the most common reasons people seek care from an oral and maxillofacial surgeon is to evaluate an oral lesion or mass. Of course, everyone’s primary concern is whether the lesion is oral cancer. Many patients are initially very anxious about the consultation; some even avoid making an appointment due to anxiety. Hopefully, this article will discuss the most common types of oral lesions, which are mostly benign, and ease patients’ minds.
The most common lesion in the mouth is Leukoplakia. It is not a pathological diagnosis but a clinical diagnosis of a non-specific white lesion. White lesions such as hyperkeratosis, scar tissue and fibromas are generally benign. Hyperkeratosis is a thickening of the skin due to irritation, such as calluses on the knees and elbows. It appears white intraorally due to the wet environment. Scar tissue and fibroma form from the trauma extending below the mucosa or skin, which causes repairing cells called fibroblasts to put down too much collagen.
Another common mass in the mouth is Torus. It is a benign bony formation on the roof of the mouth and underneath the tongue in the lower jaw. Many patients and even some doctors were alarmed that it could be bone cancer, but it is only a benign, slow-growing bone; 90% of these are bilateral. Many Tori are diagnosed without a biopsy. Sometimes it needs to be removed because it interferes with denture fabrication, leading to pain when wearing the denture.
The main concern for an oral maxillofacial surgeon is the presence of red lesions or ulcers in the mouth. A red lesion is called Erythroplakia, and if a patient has a history of tobacco use, diabetes mellitus, or is immunocompromised, a biopsy would be warranted. A biopsy involves injecting a small amount of local anesthetic into the area and removing a small tissue sample for a pathologist to evaluate. Of course, neck swelling can represent lymph node involvement, suggesting possible malignancy.
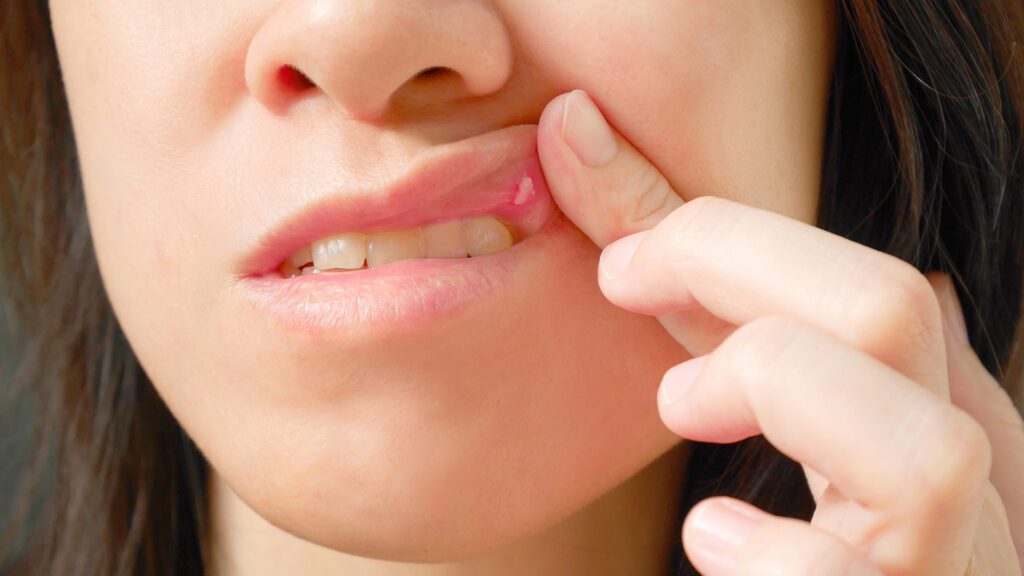
For intra-oral ulcers, I am more concerned with long-term non-healing and enlarging ulcers. The most common type of oral ulcer is an aphthous ulcer, which is benign. Its cause is unknown, but we know it is associated with increased stress and local tissue trauma. The good thing is that symptoms are self-limited for about two weeks and require no intervention in most cases. People are familiar with recurrent herpetic labialis, called canker sores. It is also self-limited for about two weeks in most cases.
If a lesion or mass is blue, it is most likely caused by an enlarged vessel, such as a Varix. It is an enlarged and engorged small vein that appears blue due to engorged blood. Usually, it is removed for cosmetic reasons in the office, with few complications. The concern for melanoma in the oral cavity is very low, as cases are extremely rare, approaching the level of microscopic detection. I have only seen it once in my career.
Many of these lesions are detected by your general dentist or hygienist during your routine annual or bi-annual visits, which is another reason you should seek regular dental care. Patients are referred to oral & maxillofacial surgeons to evaluate a lesion that your general dentist cannot quickly diagnose. To ease the patient’s mind, we recommend a small-office biopsy to completely rule out malignancy unless we are sure the lesion or mass is benign. If you have any concerns about lesions or masses in your oral cavity, please seek a dental professional to ease your worries.
Dr. Sung Cho earned his DMD from the University of Pennsylvania School of Dental Medicine and his certificate in oral and maxillofacial surgery from Thomas Jefferson University Hospital. He is currently a clinical assistant professor at Rutgers School of Dental Medicine.